Thinking About Treatment Planning Through a Depth-Oriented Lens
Treatment plans can sometimes feel like they require us to reduce rich human experiences into checkboxes, symptoms, and behaviors. Many clinicians who are drawn to relational, attachment-based, psychodynamic, experiential, or somatic approaches worry that the language required for documentation asks them to work from a fundamentally different philosophy than the one they actually practice.
So how do we work with this requirement?
A treatment plan is not a description of everything that happens in therapy. It is an administrative document that communicates medical necessity, identifies the areas of functioning most impacted by a client's symptoms, and provides a roadmap for how treatment will support meaningful improvement. The treatment itself remains deeply human, relational, and responsive.
Rather than viewing these two perspectives as competing, I encourage you to think of treatment planning as translation.
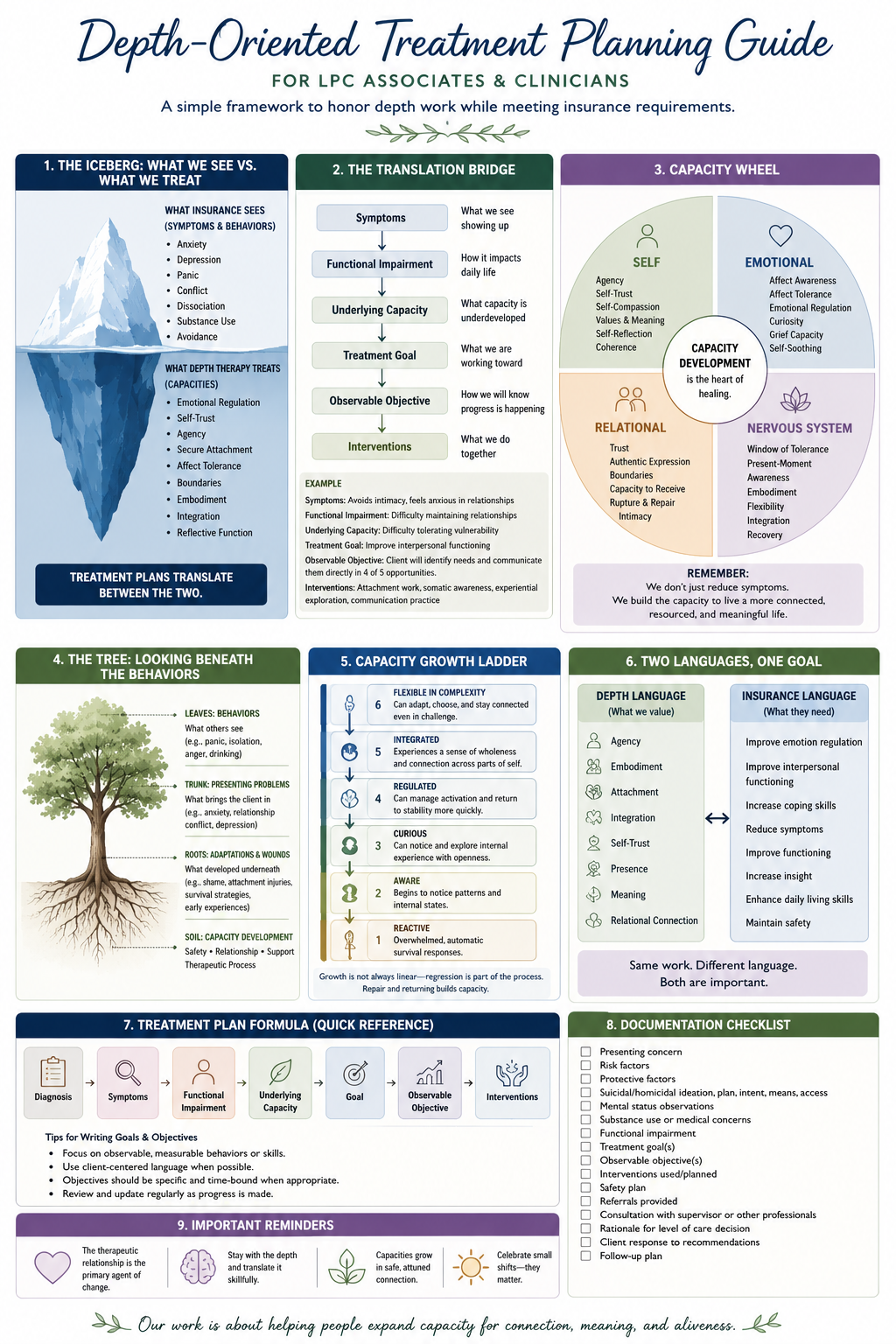
Insurance companies generally ask:
What symptoms are present?
How are these symptoms impairing functioning?
What measurable changes are expected?
Depth-oriented therapy asks:
What capacities has this person had to sacrifice in order to survive?
What developmental or relational processes have been interrupted?
What capacities, when strengthened, will naturally reduce symptoms and improve functioning?
These are not opposing questions. They are different ways of describing the same process.
When writing treatment plans, begin by understanding the client's symptoms and how they interfere with daily life. Then ask yourself a second question:
What capacity needs to grow for these symptoms to soften naturally?
For example, chronic anxiety may be rooted in limited capacity to regulate emotional activation. Relationship conflict may reflect difficulty identifying needs, setting boundaries, or remaining connected during moments of vulnerability. Depression may involve diminished agency, self-compassion, or connection to meaning. Dissociation may indicate that remaining present with overwhelming experience has not yet become sufficiently safe.
Our work is often centered on developing these deeper capacities. The treatment plan simply communicates this work using observable, measurable language.
As you write goals and objectives, remember the following principles:
Focus on Function
Insurance is interested not only in symptoms, but in how symptoms interfere with important areas of life. Consider how the client's difficulties affect relationships, work, parenting, school, self-care, decision-making, or daily functioning.
Write Objectives That Can Be Observed
Capacities themselves are not directly measurable, but their expression is.
Instead of:
Increase self-trust.
Consider:
Client will identify personal needs and communicate them directly in interpersonal situations.
Client will make values-based decisions with reduced reassurance seeking.
Client will identify internal emotional experiences with increasing specificity.
These observable changes reflect deeper developmental growth while remaining appropriate for documentation.
Interventions Describe What You Do Together
Interventions should reflect your actual therapeutic orientation whenever possible. Examples include:
Attachment-focused exploration
Experiential interventions
Somatic awareness and regulation
Psychoeducation
Mindfulness
Reflective questioning
Relational processing
Parts-oriented interventions
Emotion-focused interventions
Cognitive restructuring, when appropriate
Skills development, when clinically indicated
You do not need to abandon your theoretical orientation in order to satisfy documentation requirements. Instead, describe your work in language that demonstrates how it supports symptom reduction and improved functioning.
Remember What We Are Really Measuring
Although treatment plans often emphasize symptoms and observable outcomes, the deeper work of therapy is the gradual expansion of human capacity.
As capacity grows, clients often become more able to:
remain present during emotional activation,
identify and communicate their needs,
regulate difficult emotions,
tolerate vulnerability,
establish healthy boundaries,
reconnect with agency and self-trust,
recover more quickly following distress,
and engage more authentically in relationships.
These shifts frequently lead to symptom reduction—not because symptoms were directly targeted, but because the underlying capacities needed for healing have strengthened.
Our role as therapists is to support this developmental process. Our role as clinicians is to document it clearly enough that others can understand the medical necessity of the work. Thoughtful treatment planning allows us to do both with integrity.